An Equity-driven Analysis of the Implications of Attachment and Attachment Readiness within Primary Care Healthcare Systems in Canada
What is this research about?
Millions of Canadians don’t have a family doctor or nurse practitioner. This study looks at why simply registering people for or attaching them to primary care isn’t enough to fix the problem. Researchers outline the importance of attachment readiness. They sought to identify challenges and barriers to meaningful healthcare relationships. They explore how connecting a patient to a primary care provider only works well when the patient, the provider, and the healthcare system are all prepared for that relationship to succeed.
The study was guided by three main questions:
- What do “attachment” and “attachment readiness” refer to in primary care?
- What is the cost to the healthcare system when patients are attached without being properly prepared, or not attached at all?
- What helps at patient, provider, and system level, and what gets in the way of attachment readiness?
This report is written in the context of Ontario’s Primary Care Action Plan, which aims to attach 1.8 million Ontario residents to primary care, primarily by funding the creation and expansion of interprofessional primary care teams by 2029.
What do you need to know?
Despite many efforts, millions of Canadians remain unattached to a consistent primary care provider that negatively affects the Canadian economy in multiple ways. About 6.5 million Canadians (more than 15% of the population) don’t have a regular primary care provider. Canada ranks near the bottom among wealthy countries for primary care attachment rates. This gap hits some groups harder than others, including newcomers (immigrants and refugees), low-income individuals, people who’ve been incarcerated, people with a history of opioid use, and people facing mental health challenges. Without a regular provider, people tend to rely on walk-in clinics and emergency rooms, which leads to fragmented care, missed referrals, and worse health outcomes over time.
Across Canada, the shortage of primary care providers is bleak. About 23,000 family doctors are needed, but only 1,700 new graduates enter the workforce each year. Provinces have launched centralized waitlists and matching programs (Ontario’s Healthcare Connect, BC’s Provincial Attachment System, Quebec’s Guichet d’accès are some examples), but these systems mostly treat attachment as a simple yes/no administrative event. A patient is either matched or not.
What did the researchers do differently?
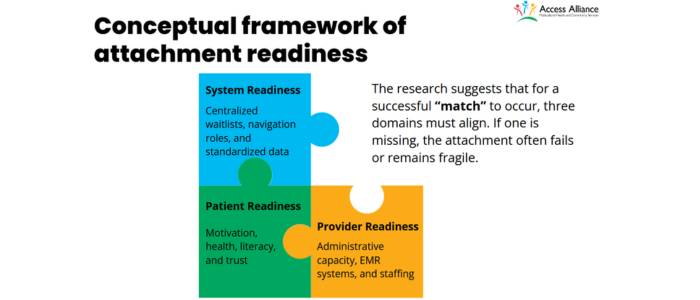
What makes this study unique is that it challenges that binary view. Rather than just counting how many people get matched to a provider, researchers suggest attachment needs to be understood as a process that unfolds over time. True attachment is a function of attachment readiness, a relational process shaped by the intersection of patient preparation, provider capacity, and systemic support. It is shaped by whether patients are ready and supported, whether providers have the capacity to take them on, and whether the surrounding system helps or hinders the connection.
What did the researchers find?
‘Attachment Readiness’ is not a singular attribute or a personal trait. It is a multi-level, ongoing condition shaped by patients, providers, and system design working together. When any one of these three pieces is fragile or missing, the match to a provider often fails.
This study and analysis were conducted using data on Ontario residents; however, they have significant implications for equity-deserving populations such as newcomers, refugees, and people without status. Across jurisdictions and health system models, attachment readiness emerges as a relational, process-oriented, and context-dependent construct.
From patients, the study found that even highly motivated people trying to get a family doctor were worn down by long waits (reported wait times ranged from one to seven months), confusing communication, and having to repeat the same information repeatedly. This erodes trust over time; a pattern the researchers call “readiness decay.” As researchers note, unattached patients experience frustration, disengagement, and reduced trust the longer the process drags on. They outline, on the positive side, that patients said their readiness was strengthened when staff showed empathy and patience, arranged interpreter support, and gave enough time during the first visit.
From primary care providers, onboarding new patients involves a large amount of unpaid, invisible administrative work, such as creating charts, verifying insurance, and tracking medical records. This work competes directly with time spent on patient care. This often results in providers limiting who they’ll accept, favouring simpler cases over patients with complex needs.
From program managers, readiness was described as something that needs to be approached with a system mentality, through holistic engagement and stabilization rather than discrete onboarding events. Roles like nurse concierges or health system navigators who prepare patients and gather information before the first doctor visit are essential. These roles and interventions ease the burden on primary care providers, improving the chances of a lasting match. Researchers outline the characteristics of an attachment-ready primary care provider. Implementing these characteristics requires adequate system infrastructure investments. In this model, readiness is developed through sustained engagement rather than immediate physician attachment.
Even a well-matched, motivated patient can lose momentum and disengage if the process takes too long — something the researchers say has been largely overlooked in past attachment policies. This matters because it suggests that current systems that focus solely on increasing the number of “matches” may be missing the real reason many attachments fail or don’t last.
Researchers suggest that attachment to primary care is one leg of a three-legged stool, upheld and sustained by the two others – equity and access. To facilitate true attachment and to move beyond fragmented care and reliance on high-cost emergency departments, healthcare policymakers must consider attachment readiness by standardizing onboarding, adopting an equity lens prioritizing vulnerability, and supporting provider capacity to build relationships for patients with complex needs.
How can you use this research?
For healthcare policymakers (provincial and federal): The study recommends moving away from measuring success by enrollment numbers alone and instead tracking “Readiness Indicators” as leading measures of whether attachment efforts are working. These measures include the time from registration to a completed intake, and patient-reported preparedness scores. Researchers also encourage policymakers to fund the identified attachment-readiness characteristics to ensure successful attachment. This includes standardized digital intake systems across clinics to cut down on repetitive paperwork, and to build equity considerations (like clinical urgency and social determinants of health) into centralized waitlist algorithms rather than relying on simple first-come, first-served ordering.
For community health organizations serving newcomers, refugees, and equity-deserving populations: The findings highlight that these populations face the greatest risk of “readiness decay.” Proactive outreach, interpreter support, and culturally responsive onboarding are especially important tools to prevent people from falling through the cracks during long wait periods.
For primary care organizations and clinic managers: The findings point to real value in creating dedicated “navigator” or “concierge” roles to handle onboarding tasks like collecting patient histories and coordinating records before the first physician visit. This reduces the administrative load on providers and was linked to higher patient satisfaction in the study’s own pilot comparison. Clinics are also encouraged to build multiple ways for patients to communicate (not just phone or email), since digital-only systems can shut out patients with limited digital literacy. While primary care providers serving equity-deserving communities are encouraged to incorporate culturally responsive services and onboarding, in a diverse province all primary care providers must incorporate culturally safe patient navigation supports and culturally responsive outreach and engagement.
For primary care providers (physicians and nurse practitioners): The research suggests advocating for financial and administrative incentives that reflect the real labour involved in onboarding complex patients, since current remuneration models often don’t account for this work, discouraging providers from accepting patients with more complex health and social needs.
What did the researchers do?
The study used a sequential mixed-methods design, combining a literature review with interviews.
Step one: Scoping review. The team searched five academic databases (PubMed, MEDLINE, ProQuest, ScienceDirect, and JSTOR), plus Google Scholar and grey literature sources like government reports. Out of 86 studies found after removing duplicates, 48 were screened, and ultimately 24 peer-reviewed articles and 10 grey literature articles were included. Most of these (58% of peer-reviewed and 90% of grey literature) focused on Canada, with the rest drawing on comparable health systems in Iran, the Netherlands, New Zealand, France, China, and Indonesia.
Step two: Qualitative interviews. Between October and December 2025, the team conducted semi-structured, in-depth interviews with 13 participants: 8 patients, two physicians from private clinics, one physician from a community health centre, and two program managers. Patients were recruited through the Access Alliance Multicultural Healthcare Centre, either by phone or in person, and were eligible if they had recently gone through the process of trying to attach to a primary care provider. Providers and staff were recruited through professional networks and email invitations, and needed to have direct experience with patient intake, onboarding, or panel management. Interviews lasted 30 to 60 minutes, were audio-recorded with consent, and were analyzed using a thematic coding approach to identify recurring patterns across the different groups of participants.
Step three: Validation. The findings from the scoping review and interviews were checked against each other and further validated through expert consultation, strengthening confidence that the patterns identified — particularly around readiness as a multi-level, process-based condition — held up across both the published literature and real-world Canadian experiences.
The authors are upfront about some limitations: only English-language sources were included, most included studies focused on Ontario and Canada (limiting how well the findings generalize elsewhere), and the small number of qualitative interview participants means not all perspectives may be represented.
Further reading
Authors: Akm Alamgir, Subrana Rahman, Saleema Allana, Rosanra Yoon, Kasia Filaber, Cliff Ledwos, Pema Yanzom, Faye Goldman, Michelle Naimer, Jennifer Rayner
Related Access Alliance work
Scaling equity-based attachment means being ready for more than just matching
As we move towards Ontario’s 2029 primary care attachment goal, we face a choice. We can build an attachment system based strictly on administrative matching by counting numbers. Or we can build a system that invests and values engagement, access, and equity equally, to create true attachment based on readiness, relationships, and structural supports. We recently conducted a study that advocates for a policy shift toward standardized onboarding and navigation infrastructure to ensure equitable, sustainable, and longitudinal care.
Advancing health equity, strengthening attachment readiness, and improving mental health outcomes for Black children and youth
Access Alliance’s annual Community-Based Research Retreat Day in 2026 focused on advancing health equity, strengthening attachment readiness and systems of care, and improving mental health outcomes for Black children and youth community members. In the morning, we focused on advancing health equity through attachment readiness and systemic transformation. Attachment to primary care is like one leg of a three-legged stool. It is upheld and sustained by the two others: equity and access. Attachment is a system-enabled relationship rather than a singular administrative event. To achieve sustainable continuity of care, we need a readiness-informed approach to attachment that invests in navigation supports, reduces clinician burnout, and standardizes intake processes. Watch presentation and panel discussion videos from the event.
Evidence-driven equity: Turning community knowledge into healthier, fairer systems for immigrants and refugees
The 2026 Annual Research Impact Report of the Community-Based Research (CBR) and Evaluation Department at Access Alliance presents a compilation of our team’s scholarly contributions, methodological advancements, and initiatives from April 2025 to March 2026.